Skin cancer is one of the most common cancers, with several million cases diagnosed per year. While many skin lesions are harmless, certain changes in appearance or behavior may indicate the presence of a cancerous or precancerous growth. Early diagnosis and appropriate treatment are important in preventing deeper tissue involvement and the need for more complex surgical care.
At McKinnon Plastic Surgery, skin cancer treatment is provided by Dr. McKay McKinnon, a board-certified plastic surgeon and member of the American Society of Plastic Surgeons and the American Society of Craniofacial Surgeons. His practice emphasizes careful diagnosis, precise surgical removal of suspicious lesions, and reconstruction techniques that preserve both function and appearance.
Signs A Skin Lesion May Need Medical Evaluation
Not every skin lesion requires medical attention, but certain changes may indicate the need for evaluation by a physician.
A lesion should generally be examined if it:
- Continues to grow over time
- Appears unusual compared to other marks on the skin
- Causes bleeding or breakdown of the skin
- Appears darker than the surrounding skin
- Becomes raised or changes in shape or texture
Some patients also choose to remove moles or other lesions for cosmetic reasons. In those cases, removal is typically a minor office procedure performed under local anesthesia.
Why Surgical Removal Is Often Recommended For Skin Cancer
When a lesion is suspicious for skin cancer or has been confirmed by biopsy, surgical excision is often the most reliable treatment. Removing the lesion surgically allows the tissue to be examined by a pathologist to confirm that the cancer has been completely removed.
Treatments such as liquid nitrogen freezing may appear convenient because they can be performed quickly. However, freezing can leave cancer cells deeper in the skin, which may allow the tumor to recur later. Surgical excision provides the advantage of confirming clear margins and ensuring the lesion has been fully removed.
Where Skin Cancer Removal Is Performed
The location of treatment depends on the lesion’s complexity and location.
Office-Based Removal
Many skin cancers can be safely removed in the office under local anesthesia. This is commonly done for lesions located on areas of the body other than the face.
After removal, the specimen is carefully marked and sent to a board-certified pathologist to confirm the diagnosis and determine whether the margins are free of tumor. Patients typically return only for suture removal and a wound check.
Hospital-Based Treatment For Complex Lesions
Cancers involving the face, scalp, ear, or neck may require hospital treatment. In this setting, a pathologist may examine the specimen during the procedure to determine whether the entire tumor has been removed.
Once clear margins are confirmed, reconstruction of the surgical site can be completed during the same procedure. This approach often allows patients to return home the same day without the need for additional surgery.
Surgical Reconstruction After Skin Cancer Removal
Some skin cancers require reconstruction after the tumor has been removed. Reconstruction techniques vary depending on the size and location of the surgical defect.
Plastic surgeons are trained in methods designed to restore both function and appearance, particularly when cancers occur in visible areas such as the face, scalp, or ears. Careful reconstruction can help preserve normal contours and minimize visible scarring whenever possible.
Frequently Asked Questions About Skin Cancer Treatment
Why Choose McKinnon Plastic Surgery For Skin Cancer Treatment?
Skin cancer surgery often requires both precise tumor removal and thoughtful reconstruction, particularly when lesions occur on the face, scalp, or ears. Dr. McKay McKinnon is a board-certified plastic surgeon with decades of experience in reconstructive surgery, including procedures involving delicate facial structures and soft tissues.
In addition to his clinical experience, Dr. McKinnon has held academic appointments, including Clinical Assistant Professor of Surgery at the University of Chicago, reflecting his longstanding involvement in surgical education and complex reconstructive care. His training and experience allow him to manage both the removal of the tumor and the reconstruction of the surgical site when needed.
This combined approach helps ensure that patients receive treatment that addresses both the medical problem and the long-term functional and aesthetic outcome.
Skin Cancer Treatment In Chicago, IL & Coral Gables, FL
Skin cancer treatment often involves careful surgical removal of suspicious lesions and reconstruction of the affected area when necessary. Patients in Chicago, IL, and Coral Gables, FL, who have concerns about a changing or suspicious skin lesion can contact McKinnon Plastic Surgery at (312) 335-9566 in Chicago or (305) 753-1400 in Coral Gables to schedule a consultation.
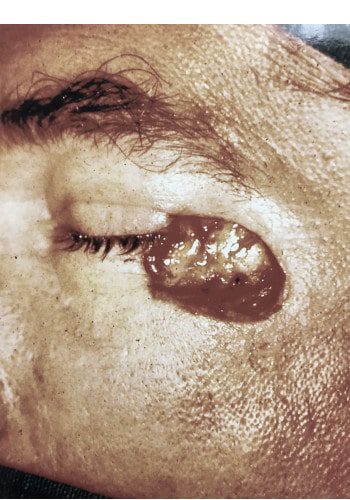
Front: Resection and reconstruction of basal cell carcinoma.